Physician Integration Along the Patient Safety Spectrum: From Pre-School to PhD
Introduction
The hospital risk manager exclaimed, “I have good news and I have bad news. The good news is we have just employed 1,000 physicians. The bad news is we have just employed 1,000 physicians! How do we begin the process of onboarding and integrating them into our culture from a risk, safety and quality perspective?
“Where do we start? Is it basic risk blocking and tackling: the elements of a medical malpractice action, communication and handoffs? When do we get to cyber risk, EMTALA, HIPAA, Just Culture, teambuilding… quality metrics and programs for the highest risk specialties? Help!”
TSG has been asked that question at so many conferences and trade shows we decided to take a structured approach to providing an answer. We have reached out to several very well-known veteran risk, safety and quality leaders about their experience in physician integration and onboarding and asked them to “take us to school.” Rather than give you the TSG version, here is the story from four very different organizations at various stages of physician integration.
But before we begin, let’s take a peek from 20,000 feet. Why has this become an issue in the first place? The drivers for clinical integration have been well published in white papers, journals and the press. There is general agreement as to why integration is occurring, but there is a broad spectrum regarding how and to what extent it is happening.
Without getting lost in the weeds, there is a new reimbursement paradigm that requires a new construct, a new organizational structure. It is time to pave the way for quality and value-based reimbursement, and that requires a fundamental transition in the structure of healthcare delivery.
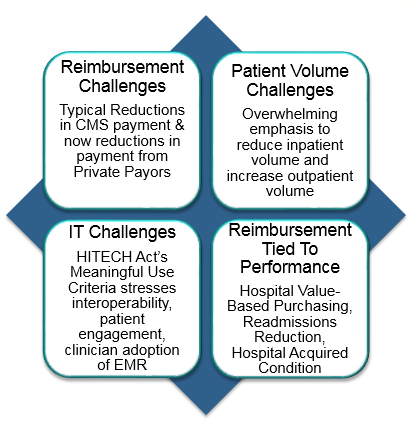
Why own physician practices? In the not too distant future, it will not be possible to divvy up the fee-for- service pie. The performance-based reimbursement world will require a close integration of the medical staff. Integration will be necessary from a cost and a functional perspective.
Within the new paradigm, there will be winners and losers. The winners will have integrated with clinicians and maintained or increased market share through practice ownership or integration. The winners will coordinate with clinicians to maintain or grow revenue under Value-Based Purchasing, HAC, HCAHPS, readmissions reductions, and the quality-based incentive or penalty de jour.
Hospital leadership working with clinicians as a single team for patient safety, for risk reduction, for reducing variability in care and medical errors, and achieving quality metrics will live to tell the tale. Hospital organizations that are not preparing for the inevitable will see market share go elsewhere: higher costs, loss of incentives, stiff penalties and loss of already thin margins.
So let’s hear from our well-known risk and quality leadership. What did they do? How did they accomplish it? How long did it take? What are the keys to success?
Question to Hospital System:
“I am curious, as health systems employ or create closer relationships with the medical staff, sometimes taking responsibility for insuring those practitioners, what educational efforts have you made to level set or what are the most significant or current pain points, problems, risks? If you could wave your wand and get them all on board with understanding certain key issues, spanning all specialties, what would you want them to know or be aware of?
“Would it be keys to successful communication (documentation essentials, handoffs…), satisfaction, cyber risk, common medication errors, risk and the EHR, more general medicolegal issues? I am just naming a few to initiate the thought across. What are the biggest pain points across the continuum for you?”
Organization #1
This is a short story! This organization is a recent 40-hospital spin off from a very much larger organization. The new organization started life within the last 6 months. We knew that not much could have been accomplished, but were wondering about plans for the future.
“So Mr. J, I sent you an outline of the subject of today’s discussion points and wondered if you had given it any thought.”
“Well Dr. D., I have given it some thought. As of six months ago I took on responsibility for 400 employed physicians, and honestly I have no idea yet what the integration strategy will be. I still don’t know who we insure and what docs have their own insurance. We are still addressing the basic fundamentals of starting a new organization and have a ways to go. I do see a captive insurance company in our future, and within the next 6 to 8 months we will be working out our strategy for developing the kind of culture you are asking about. As I have done with prior organizations, I hope to fund some of our risk and safety programs out of the captive, but that will take some time.
“We will begin programming in the highest risk specialties including OB, ER and Surgery, and will look for educational opportunities in the marketplace as well as internal development. We will develop playbooks for key risk and safety and will implement them across the enterprise as I have done in other organizations.
“But we are just at the beginning of that journey and have a long road to go.”
Organization # 2
“Dr. A, have you had an opportunity to review our questions on physician integration and onboarding. If so, perhaps you would share your vision and recount some of your successes and challenges in this changing medical marketplace.”
“Dr. D., yes, and we are happy to engage in the discussion. I am the Chief Medical Officer, and joining me are our VP of Risk and VP of Quality.
“We decided upon an integration strategy approximately two years ago and have been actively employing physicians and purchasing clinic practices. We feel that is a key to maintaining market share in our communities and reducing duplication of administrative services and lowering costs. We are a Midwest organization with approximately 17 hospitals and 300 clinics in a three-state area. We now employ 900 physicians.
“What an organization will need in terms of physician integration depends in large part on their stage in the developmental spectrum. We have just now gotten our arms around the basic new structure, and our current focus is dealing with basic risk and quality issues across all specialties. We think of this stage of the process as ‘onboarding,’ and we are looking for liability basics. We have decided to implement a curriculum of general risk-related issues and will make that education mandatory for all employed physicians. We will probably provide a menu of 5 to 10 important risk subjects and require the physicians to choose an agreed upon number of those.
“Our current general areas of concern are as follows, in no particular order:
- Risk nuances related to Electronic Medical Records
- Handoffs in care – ED to Hospitalist, inpatient to nursing home, etc.
- Virtual space work – we provide 24-hour care utilizing a telehealth network
- Helping providers understand what creates risk
- Documentation essentials
- The decision-making process – avoiding cognitive errors
- Transition in care errors
“The organization will also develop specific strategies for the highest risk service lines – specifically programs in Emergency Medicine, OB and Surgery.
“We look forward to the process, and view this as a work in progress and expect significant evolution over the years.”
Organization #3
“Mr. S., I know from discussions we have had over the years that you began a transition process some years ago. Can you share your thoughts about the road you have been on?”“Absolutely. We began this process approximately five years ago. The need for a new construct was apparent and we began aggressively employing physicians and buying physician practices. As a part of the new paradigm, we knew that we needed to focus on population health, and that our attention to wellness represented high-quality care, and in the long run could dramatically reduce the cost of healthcare. We also recognized that our inpatient census would inevitably decrease as our outpatient census increased, and that transition is well under way.
“In addition, our market on the East Coast is incredibly competitive, and we felt an urgency to get out there early and bring the physician practices into our organization. Yesterday physicians were on staff at multiple hospitals. In the new paradigm, physicians will increasingly integrated into a single health system, although there will be some variation on that theme.
“For the first two years we were just out there hiring, and now employ approximately 2,000 physicians. We needed a critical mass to achieve success. The next two years was about how to manage. From a human resources and administrative perspective, it was about contracts, retention, and getting the right team on the bus.
“We decided that within the employment model, that there should be limited variability in contractual relationships. All practitioners are on a salary plus incentive and have a 5-year employment agreement with penalties for early termination.
“The incentives relate to a range of risk and quality goals as well as the financial viability of the organization. That includes patient volume, RVUs, quality (although this is less well defined but will become more meaningful over time), safety, and patient satisfaction.
“We decentralized the organizational structure and created a medical group to represent the employed physicians. Through a variety of mechanisms, the medical group is very connected with organizational leadership.
“As we approached our fifth year, we decided that it was time to address clinical excellence, quality, reducing variability in practice, meeting the standard of care, following the evidence. For example the Ortho group standardized the approach to joint surgery across all providers, including technique, hardware, and antibiotic use based on the best evidence.
“The medical group then assembled into clinical practice groups. So for example, Cardiovascular, Ortho, Neuro and ED are organized into practice groups, each with clinical practice leaders.
“It may make sense early on to educate practitioners across the spectrum with enterprise-wide-type issues such as the basics of medical malpractice, insurance coverage, transitions and handoffs, EMTALA, HIPAA, and other such issues. However, in order to achieve compliance with quality metrics and more importantly reduce variability, reduce the failure to diagnose, and to standardize based upon medical evidence, it was important to create a working group for each specialty. Standardization of clinical practice and reducing variability has to come from the clinicians in close association with leadership.
“Interestingly, clinical leaders have begun asking for hard information on adverse outcomes, incidents and issues in particular specialties. They are using this information to focus on specific issues and individuals. They are truly buying into this culture.
“In the future we will continue to work on our culture - who we are, what we represent as a system. We are working very hard to create a culture where administration and clinicians work together on the same team. There are quarterly meetings between medical and administrative leadership. We make an effort at creating transparency between all leadership groups.”
Organization #4: Last But Not Least
Our final discussion was with a national organization that has utilized an employment model from its inception. They have well over 10,000 employed physicians.“Mr. M., you probably have the most mature employed physician model in the country. Can you share with us your approach to integrating new practitioners and how to keep the existing clinicians on board?”
Interestingly the initial response started with the organizational safety culture (see their diagram below.) This organization has invested heavily in safety culture. They first presented the organizational construct which currently includes 5 pillars of safety.
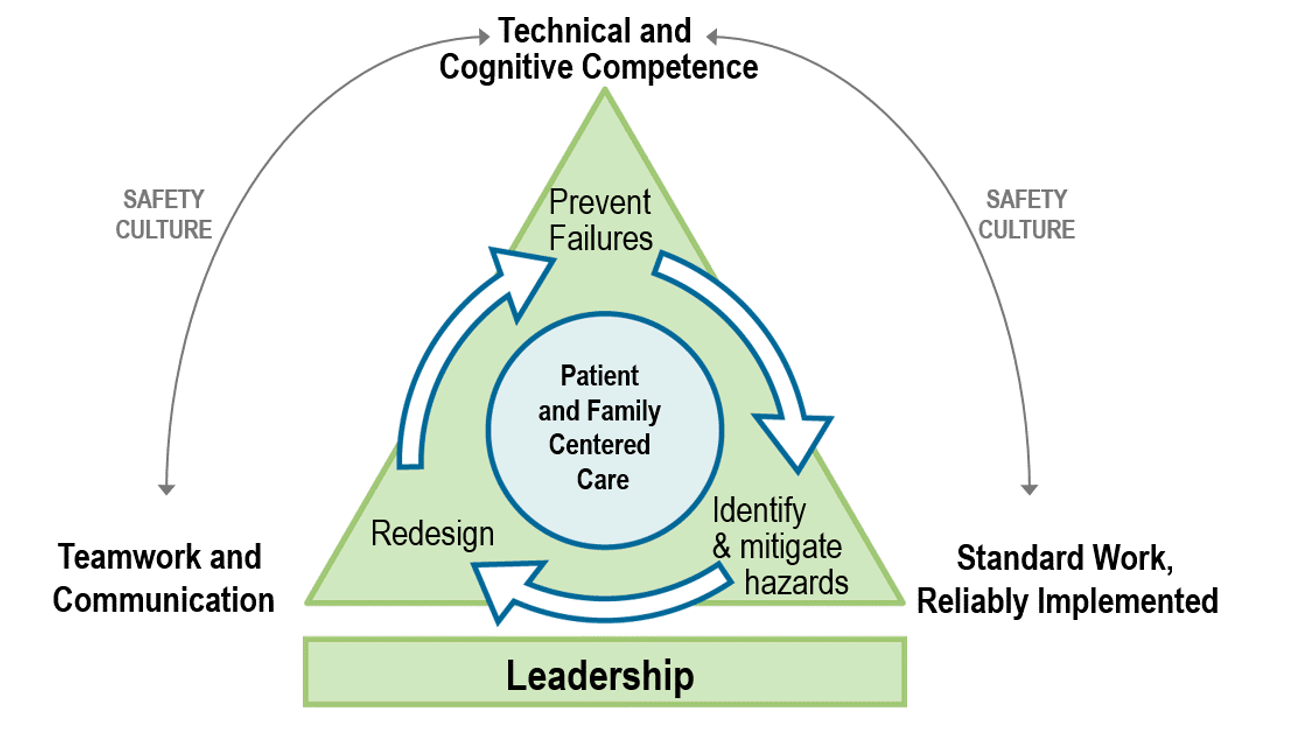
“Leadership
Patient safety is part of our culture and it starts from the top down. Safety is part of every presentation by leadership in every instance. This must be a top down priority. Leadership is at the tip of an inverted pyramid. Culture development starts with leadership and percolates into every aspect of the organization. We believe that is why they get such strong buy from front-line physicians. Safety includes work place safety, patient safety – the entire continuum.
“Patient and Family Centered Care
At the center of our construct is Patient and Family Centered Care, which has four key components:
- Dignity and Respect
- Information Sharing
- Participation in Care to the extent desired, and
- Collaboration with a subset of patients
“Technical and Cognitive Competence
Basic medical training, continuing medical education, and ongoing evaluation of competence.
“Teamwork and Communication
This generally has to be learned post-professional training. We address this through some online education and simulation.
“Standard Work Reliably Implemented
Improvement and implementation methodology. Any standardization within acceptable science is better than random variation in clinical practice because it allows us to measure deviations and outcomes and to improve. A good example is working with the best medical evidence, implementing protocols, and reducing variability in practice.
“We teach a culture of improvement. One of the keys to our Patient Safety Program is the use of our national adverse outcomes database. We have worked diligently to facilitate and expedite the process of reporting incidents and adverse outcomes to our national database. We study the database for trends and use them to develop patient safety programs.
“Generally we have the same pain points as other organizations. The failure to diagnose is probably our biggest pain point and ¾ of funded safety projects have a ‘failure to diagnose’ focus.
“Another key for our organization is a robust peer review process that is reproduced at every hospital with minimal variation.
“One of the key elements in our education is a focus on the cognitive space. That is the process by which clinical decisions are made, understanding cognitive pitfalls and human bias – heuristics. We also believe that it is important to support the decision-making thought process through decision support in the electronic medical record.
“Here is an example of a regional orientation, or onboarding or as we call it, risk 101 education for new docs. Some of this is online, some is live. All front-line staff and leadership will also attend this live every 2 to 4 years.
“The organization has multiple regions, each with a certain degree of autonomy, but we are working at creating a consistent national approach to onboarding with oversight from the national risk management team.
“Here is an example from one of the regions, but it is similar to others.
- Medical malpractice overview. Duty, breach…
- On-call requirements, obligations, potential for exposure to liability and EMTALA issues
- Med mal coverage and tail.
- Curbside consults and related issues medical legal issues
- Documentation – pearls and pitfalls. Copy and paste issues with EMRs
- Informed consent and non-delegable duty
- Disclosure and apology
- Major FTD categories; e.g., surgical mishaps
- Medical errors
- Improvement methodology
- Standardization and variability. Drift causing deviation. Explanation for deviation
- Just Culture
“We utilize outsourced education and other safety tools such as our Patient Satisfaction Program, teamwork and communication.
“Evidence-based medicine development is a joint partnership between the medical group and leadership. The development process is sponsored by and driven by the medical group. We view this as a major opportunity to standardize this nationally and close some of the variation gaps.
“That said, the organization is currently working with the recent “Free From Harm” publication from the National Patient Safety Foundation (NPSF) and considering the ‘eight pillars’ or recommendations suggested in that document (which is available online through the NPSF).”

Although a complete treatment of the NPSF “Free From Harm” publication is beyond the scope of the article, this vision statement does provide organizations with an important developmental framework. But fundamentally the NPSF vision tells us that “future progress depends on a total systems approach to safety.” Early in the transformation process (pre-school), it may be necessary to identify specific problems and pain points and identify mechanisms to prevent them. This approach may lead to meaningful change, but in isolation, does not lead to widespread holistic change (PhD).
Conclusion
This has been a fascinating and educational journey. Clearly there are stages in the transformation process, and the immediate focus will vary depending upon where on the spectrum yourorganization lies. This article describes the journey of 4 organizations that span the spectrum from a fledgling spin off to a huge mature national organization that was conceived with integration as part of its vision.
Those organizations undergoing transformation may need to start with purchasing practices, contracting and human resources types of issues. But this early approach must be coordinated with a vision to the future that takes into account culture, teamwork, and patient focus as key fundamental considerations. The organization must commit to a systems approach, addressing systems design, human failures, human factors engineering, safety culture, error reporting and analysis.
Once that construct or vision is in place, the educational and other requirements for physician integration and onboarding should, in large part, define themselves. There will always be a place for circumscribed safety initiatives in response to specific problem identification. But teaching the fundamentals of a holistic culture of safety across the spectrum will lead to the fundamental transformation required in today’s medical world.















